
Labral Repair and Shoulder Dislocation
Anatomy and function of the labrum

The shoulder is a ball-and-socket joint between the upper arm bone, which is called the humerus, and the shoulder blade, which is called the scapula. The ball is on the top of the upper arm bone and the socket is on the shoulder blade. However, the socket is not a full cup, it is a shallow depression similar to a golf tee. The socket is made deeper by a triangle of cartilage that runs in a circle around the socket, called the labrum. The labrum acts similar to a suction cup. The labrum helps to prevent the ball from slipping over the edge of the shallow socket and dislocating. Ligaments between the shoulder blade and the upper arm bone also keep the shoulder from dislocating. Ligaments are strong bands of connective tissue between bones. These ligaments attach to the shoulder blade at the labrum.
Shoulder Dislocation

The shoulder is the most commonly dislocated joint in the body. Most commonly the ball dislocates in front of the socket. The ball can also rarely dislocate behind the socket. Most dislocations occur with injuries to the shoulder such as athletic injuries, car accidents, and falls. Immediately after the dislocation, the ball must be placed back into the socket. Some people who suffer a dislocation are able to push the ball back in place themselves. In sports injuries, often an athletic trainer is able to push the ball back into place. Otherwise, doctors in the emergency department push the ball back into the socket. The shoulder can also partially slide out of place. This is called a subluxation.
Labral tears
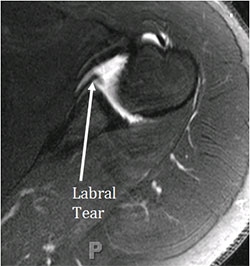

When the shoulder dislocates, the labrum in the front of the shoulder almost always tears. When the labrum tears, the ligaments attached to the labrum are no longer connected to the shoulder blade. The socket cartilage and bone can also be damaged. In severe cases, the socket can be fractured. The back portion of the ball is also almost always bruised as well. When the ball dislocates, the back portion of the ball hits the front of the socket, bruising it. This bruise can damage the cartilage. When the ball dislocates it also stretches the nerves, in rare cases this may lead to lead to nerve injuries.
Because of the damage to the ligaments and labrum with a dislocation, the shoulder is at risk to dislocate again. Overall, roughly half of all patients with a dislocation will have another dislocation. The risk of another dislocation depends upon many factors. Both young people and athletes are more likely to have another dislocation. Damage to the cartilage and bone also increases the risk for another dislocation. Damage to the cartilage also increases the risk for arthritis of the shoulder later in life. Overall, roughly half of all patients with a dislocation will have some evidence of arthritis later in life.
Treatment of shoulder dislocations
After a shoulder dislocation, non-surgical treatment focuses on physical therapy. The goals of non-operative treatment are to allow the labrum and ligaments of the shoulder to heal while strengthening the rotator cuff. The rotator cuff compresses the ball into the socket, preventing another dislocation. Often, immediately after a dislocation the shoulder will be placed in a sling for one week before starting therapy. Working with a therapist is helpful to make sure the best exercise types are used. The main muscles to be strengthened are the rotator cuff muscles. The muscles that connect to the shoulder blade can also be important and must be strengthened. During physical therapy the arm position that most commonly leads to a shoulder dislocation must be avoided. The total length of therapy depends upon the patient. Many patients are ready to transition to a home program after six weeks.
Surgery

For patients with multiple dislocations, continued shoulder pain, or for some high-risk patients with a single dislocation, Dr. Chalmers may recommend a surgery to repair the shoulder. High-risk patients are young patients (<30 years old) and those who participate in contact or collision sports. This surgery can take several forms depending upon the damage to the shoulder, and can include repair of the labrum and ligaments, which is called a labral repair, an arthroscopic shoulder stabilization, or a Bankart repair. It can also include repair of the dent in the back of the ball, called a remplissage. It can also include bone grafting of the front of the socked. Dr. Chalmers can perform all of these procedures through an arthroscopy.
In the surgery, Dr. Chalmers uses sutures and anchors. Special extra-strength sutures attach to anchors. These sutures are not absorbable, but will cover with scar tissue and do not need to be removed. Dr. Chalmers will customize your repair to best restore the damage to the shoulder.
Outcomes
Overall, arthroscopic shoulder stabilization is one of the most successful shoulder surgeries. Dislocation of the shoulder after this kind of surgery is uncommon, occurring in ~7% of patients. More than 90% of patients are able to return to their pre-injury level of play. Some patients are at a higher risk for dislocation. High-risk patients include those with damage to the ball, damage to the socket, “double-jointed” patients, young patients, and patients who are athletes in contact or collision sports. In high risk patients, as many as 70% of patients will have another shoulder dislocation. In high risk patients, Dr. Chalmers may recommend a bone grafting procedure. In addition, even if the surgery is successful in preventing another dislocation, arthritis of the shoulder can still occur later on because of the damage done with the initial dislocation.
Click here to download the PDF.
You will need the Adobe Reader to view and print these documents 